
Stanford's MedAgentBench: Why Healthcare AI Agents Still Struggle in Real Clinical Workflows
Stanford's MedAgentBench: even the top model hits only 69.67% - what that means for clinical AI.


Introduction
For years, the leading AI models in healthcare have performed impressively on medical licensing exams. GPT-4, Claude, and Gemini routinely score at or above expert human levels on the USMLE, feeding a growing belief that AI is ready to enter the clinical workflow. But scoring well on a structured exam and performing reliably inside a live hospital system are fundamentally different problems-and only recently has the industry begun to measure that distinction seriously.
Stanford University's MedAgentBench, published in NEJM AI in August 2025, represents the field's most rigorous attempt to bridge this gap. Developed by a multidisciplinary team including physicians, computer scientists, and health informatics researchers-and co-authored by Andrew Y. Ng and Jonathan Chen-the benchmark tests AI agents not on what they know, but on what they can actually do within an electronic health record environment. The results are clarifying and sobering in equal measure. This article unpacks what MedAgentBench reveals about the state of healthcare AI agents, why the findings matter for enterprise clinical deployment, and what healthcare organizations must understand before scaling agentic AI in healthcare beyond the pilot stage-and why AI agents in healthcare must now be held to a higher standard of evidence than any benchmark before it.
Why Healthcare AI Governance Matters More as Models Become More Powerful. Explore the latest insights here!
Why "Chat Performance" Is Not Enough for Clinical AI
The core premise behind MedAgentBench is deceptively straightforward: the way AI has been evaluated in medicine has been profoundly misaligned with how medicine is actually practiced.
Traditional medical AI benchmarks-USMLE, MedQA, PubMedQA-treat clinical knowledge as the primary measure of readiness. A model that can identify the correct diagnosis from a list of options or explain a drug interaction is considered capable. But real clinical care operates in a different register. Physicians interact with fragmented data systems, place medication orders through layered EHR interfaces, retrieve lab trends across months of records, coordinate referrals, and document findings in structured formats that downstream billing and care coordination depend on.
As Jonathan Chen, a senior author of the study, put it directly: "Chatbots say things. AI agents can do things." That distinction is the backbone of MedAgentBench's contribution. The benchmark asks not whether a model can explain a clinical scenario, but whether it can execute clinical tasks with the precision that real workflows demand.
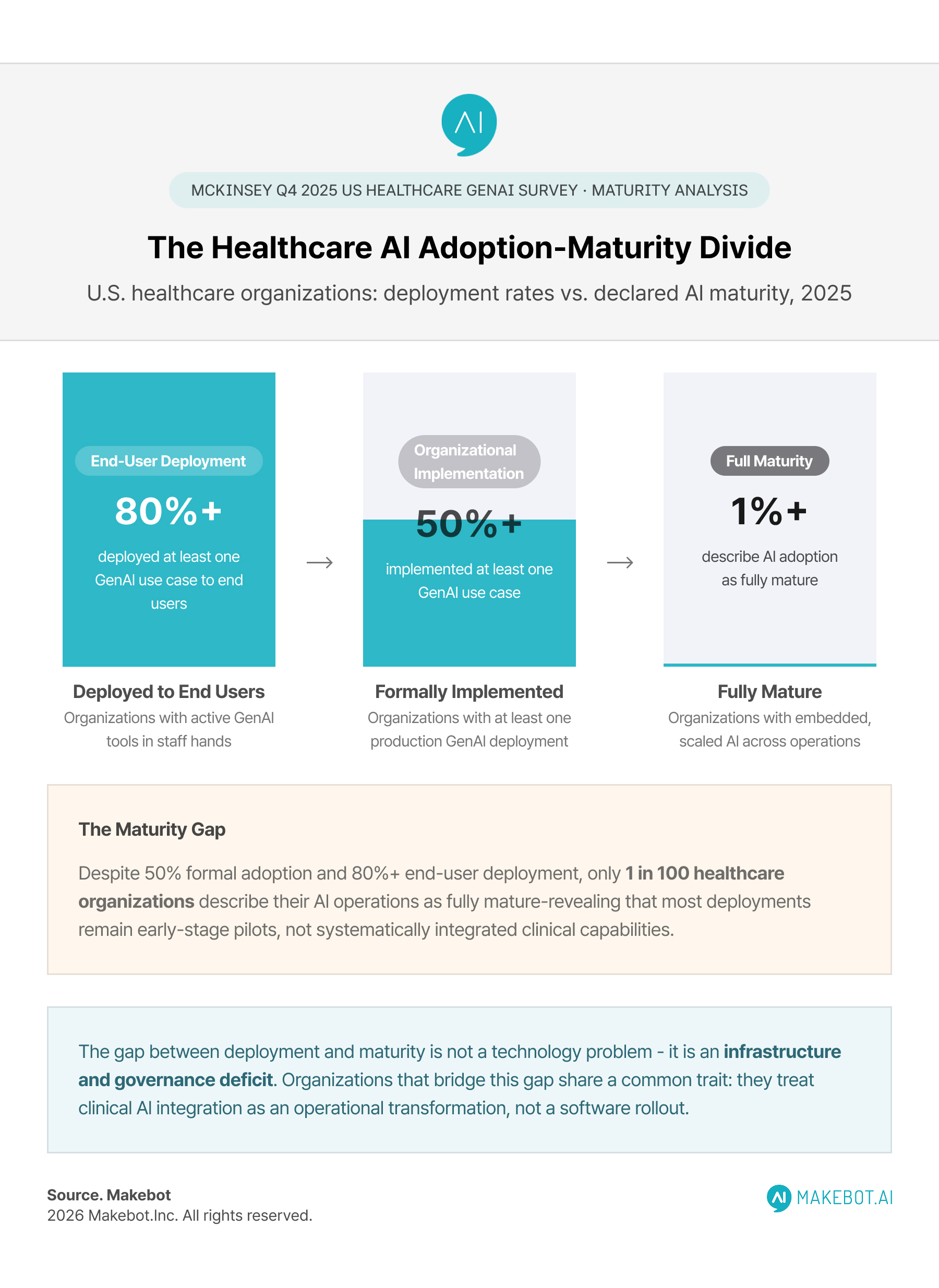
This shift matters enormously because the deployment of clinical decision support AI and autonomous clinical agents is accelerating faster than evaluation frameworks can track it. According to a McKinsey Q4 2025 survey, more than 80% of U.S. healthcare leaders report that their organizations have already deployed at least one generative AI use case to end users. Adoption has grown from 25% in late 2023 to 47% in 2024 and 50% by the end of 2025. Yet only 1% of organizations describe their AI adoption as "fully mature"-a statistic that underscores just how much of the current deployment landscape consists of early-stage pilots, often without the rigorous evaluation infrastructure that MedAgentBench is now helping to build.
How Enterprise Hospitals Are Combining RAG with GPT-5 for Safer Healthcare AI Systems. Read the expert analysis here!
Inside MedAgentBench: What Stanford Built and Why It's Different
The design of MedAgentBench reflects a deliberate commitment to realism. Rather than presenting models with decontextualized clinical questions, the Stanford team constructed a fully functional, FHIR-compliant virtual EHR environment populated with 100 realistic patient profiles and more than 700,000 clinical data elements spanning labs, medications, diagnoses, vitals, imaging, and procedures. The data was designed to be messy, incomplete, and longitudinal-mirroring the actual state of clinical data that physicians navigate every day.
Against this environment, the team deployed 300 physician-authored tasks spanning 10 clinical categories: retrieving structured patient data, reviewing lab trends, ordering imaging, prescribing or adjusting medications, documenting clinical findings, and coordinating follow-ups. Most tasks required two to three sequential steps, demanding the agent to correctly call FHIR API endpoints (both GET and POST), interpret results accurately, and produce outputs in the exact formats that downstream clinical systems expect.
The evaluation metric was equally uncompromising. Success was defined as completing the task correctly on the first attempt-mirroring real-world clinical safety expectations where a single incorrect action can have meaningful patient consequences. An orchestration layer capped each agent at eight interaction rounds and nine available EHR functions, enforcing the kind of constrained operating environment that real hospital systems impose.
This design philosophy is what makes MedAgentBench a genuine advance over its predecessors. The benchmark is not testing whether a model knows medicine. It is testing whether a model can practice medicine safely under structured, reproducible conditions.
Deloitte: 75% of Healthcare Leaders Are Scaling Generative AI to Transform Care and Operations. Discover what’s next here!
What the Results Reveal: Promising but Far from Production-Ready
Twelve leading models were evaluated across the MedAgentBench task suite. The aggregate results tell a story of meaningful capability coexisting with significant limitations.
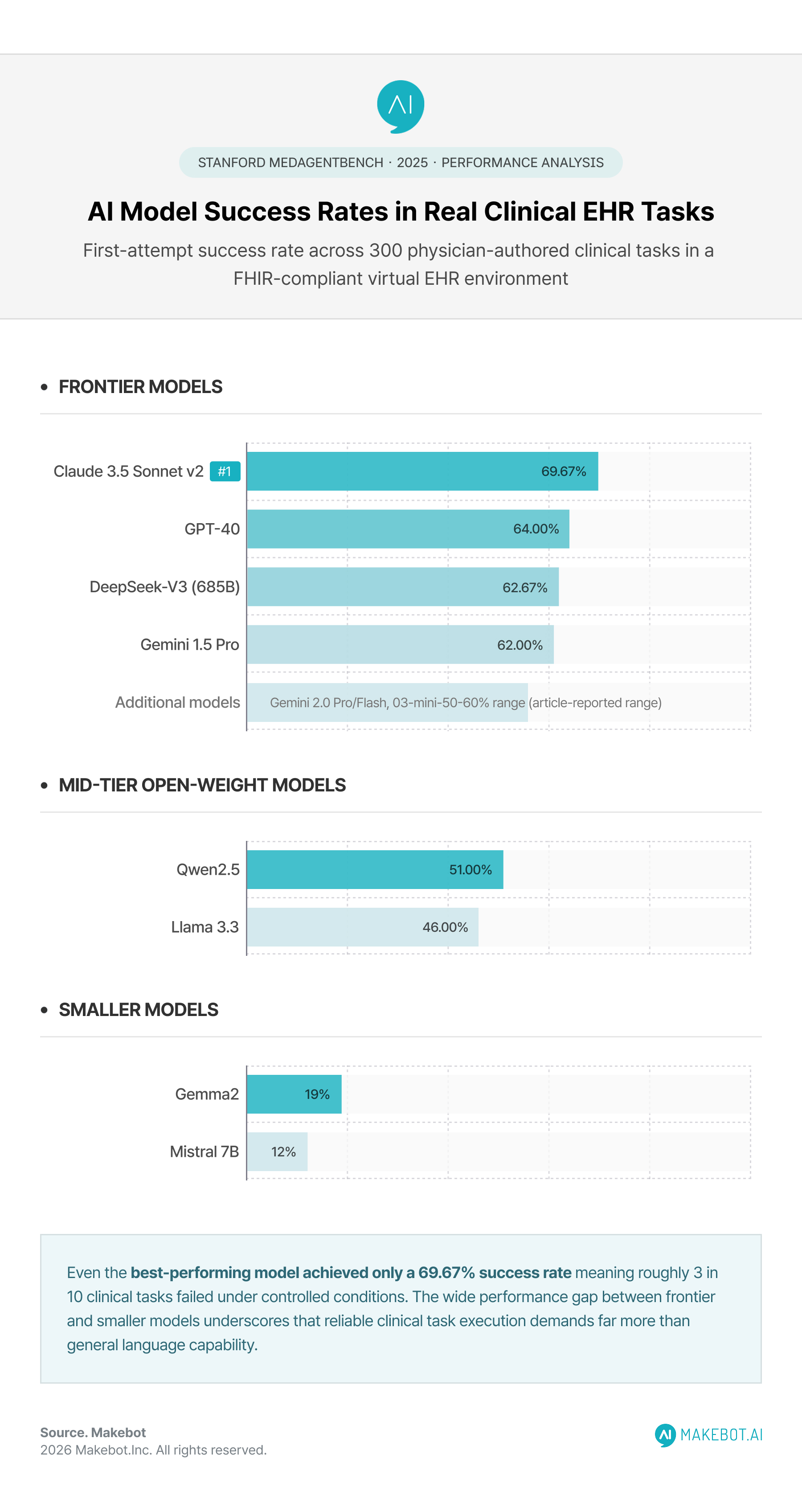
Claude 3.5 Sonnet v2 achieved the highest overall success rate at 69.67%. GPT-4o followed at 64.00%, with DeepSeek-V3 (685B) at 62.67% and Gemini-1.5 Pro at 62.00%. Mid-tier open-weight models including Qwen2.5 and Llama 3.3 ranged between 46% and 51%, while smaller models such as Gemma2 and Mistral 7B fell below 20%.
These numbers deserve careful interpretation. A 69.67% success rate, while marking meaningful progress, also means that roughly three in ten clinical tasks failed-in a controlled environment with clearly defined task parameters. In a production clinical setting, with real patients and real consequences, that failure rate is not a metric: it is a patient safety consideration.
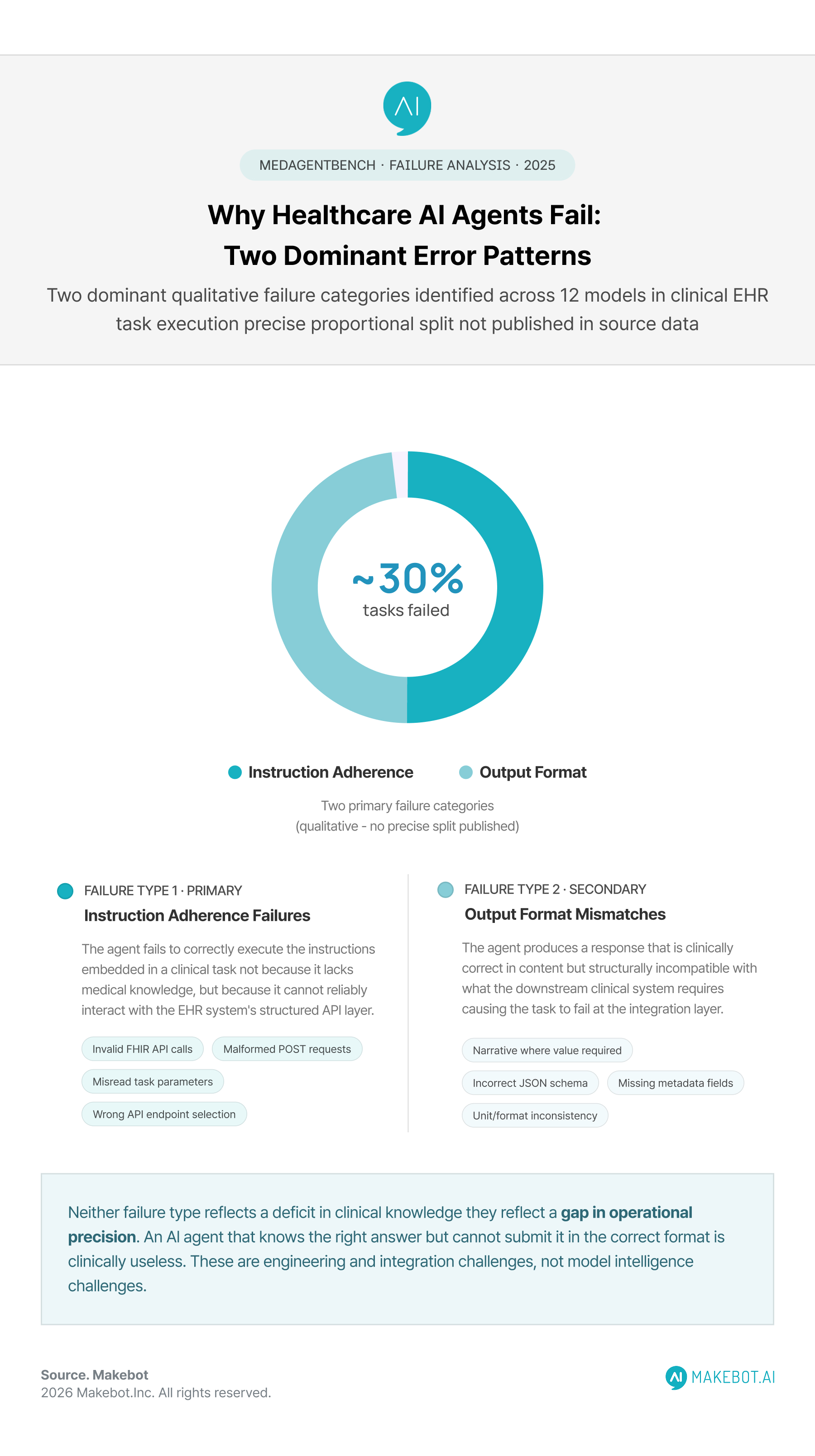
Stanford researchers identified two dominant error patterns across the models.
- The first was instruction adherence failures: invalid FHIR API calls, incorrect JSON formatting, and misinterpretation of physician task instructions.
- The second was output format mismatches: models providing narrative explanations where structured values were required, or missing mandatory metadata fields that downstream clinical systems depend on.
Neither of these failure types reflects a lack of medical knowledge. They reflect something more fundamental-a gap between language model behavior and the operational precision that clinical system integration demands. This distinction is critical for healthcare organizations evaluating where AI-powered clinical workflows can and cannot yet be trusted.
Can LLM-Powered Conversational AI Provide Safe and Effective Mental Health Support? Explore the future of AI here!
The Broader Context: Why Healthcare AI Still Struggles to Scale
MedAgentBench's findings do not exist in isolation. They reflect a pattern visible across the broader healthcare AI adoption landscape: the gap between promising pilots and reliable enterprise deployment.
McKinsey's analysis of healthcare AI in 2025 describes the industry as "caught between AI promise and peril." Most health systems remain stuck in proof-of-concept phases, struggling with integration into legacy EHR infrastructure and the operational realities of retraining clinical staff. According to Edelman's Trust Barometer data cited in McKinsey's 2025 Technology Trends Outlook, public confidence in AI providers has slipped from 61% in 2019 to just 53% in 2024-a trend that carries particular weight in healthcare, where patient consent and clinician confidence are prerequisites for meaningful adoption.
The interoperability challenge is especially acute. EHR systems like Epic-which holds between 37.7% and 39.1% of the U.S. acute care hospital market-are deeply integrated into clinical operations, but they are also notoriously complex to extend with third-party AI agents. Even in environments that support FHIR-based integration, AI agents must navigate inconsistent data structures, proprietary APIs, and governance constraints that differ across institutions. IBM's 2025 Cost of a Data Breach Report found the average healthcare data breach cost at $7.42 million-the highest of any industry for the 14th consecutive year-a figure that makes healthcare organizations justifiably cautious about expanding AI agent access to live clinical systems.
The organizational dimension is equally significant. A 2025 review of AI integration in clinical AI workflows, published in the Journal of Medical Internet Research, identified algorithmic bias, limited explainability, insufficient stakeholder engagement, and regulatory ambiguity as interconnected barriers-not isolated technical problems. Addressing one without the others does not produce reliable deployment of AI agents in healthcare.
That said, progress is measurable in targeted areas. McKinsey has documented that ambient AI scribes at Kaiser Permanente saved nearly 16,000 hours in documentation time over a 15-month period. Administrative use cases-scheduling, claims processing, clinical note summarization-have demonstrated consistent ROI where human-in-the-loop oversight remains intact. The challenge is not that healthcare AI is without value; it is that the path from point-solution success to systemic clinical workflow integration requires infrastructure that most health systems have not yet built.
McKinsey: How AI in Healthcare Can Improve Consumer Experiences. See how enterprises are transforming here!
Where Healthcare AI Agents Are Actually Working
The uneven performance landscape revealed by MedAgentBench is not a reason for pessimism-it is a map of where the work needs to happen. And even within the benchmark's current constraints, the results show that medical AI agents are already capable of reliable performance on a meaningful subset of clinical tasks.
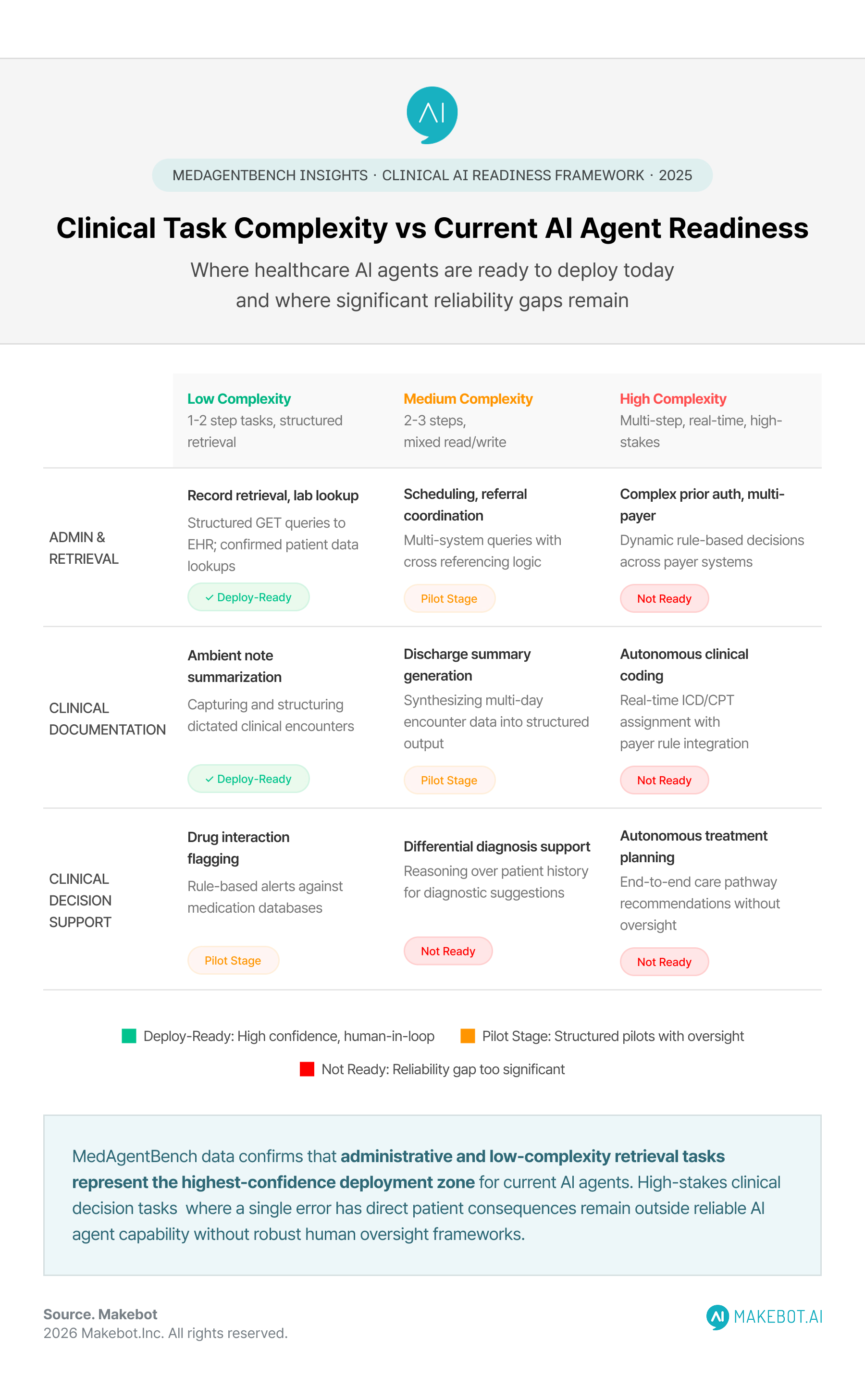
Administrative housekeeping tasks-retrieving structured patient records, checking lab results, confirming medication lists-represent a category where top-tier models achieved success rates well above 60% in controlled conditions. These are also the tasks that create the most friction in day-to-day clinical operations. Physicians spend, on average, two hours on documentation and EHR navigation for every hour of direct patient care. AI agents capable of reliably handling retrieval and documentation tasks-under human review-could meaningfully reduce that burden.
This is the vision that Stanford researchers have articulated explicitly. Kameron Black, Clinical Informatics Fellow at Stanford Health Care and a co-author of the MedAgentBench study, was direct on the matter: "AI won't replace doctors anytime soon. It's more likely to augment our clinical workforce." With a projected global healthcare staffing shortfall exceeding 10 million workers by 2030, scalable augmentation for lower-complexity clinical tasks is not a feature request-it is an operational necessity.

The industry framing is shifting accordingly. McKinsey's 2025 analysis describes a strategic pivot from stand-alone AI tools to workflow platforms-systems designed to integrate into clinical operations rather than operate alongside them. The largest healthcare AI funding rounds in 2025 reflect this direction, with clinical decision support platforms like OpenEvidence raising $410 million across two rounds as health systems look for evidence-based AI that is built for the realities of clinical deployment.
Conversational AI for Remote Patient Monitoring in Chronic Care. Learn how industry leaders are adapting here!
What MedAgentBench Means for Healthcare AI Benchmarking Going Forward
The publication of MedAgentBench in NEJM AI signals more than a new research contribution. It represents a maturation in how the industry is beginning to approach healthcare AI benchmarking-and specifically, how it evaluates AI reliability in healthcare-moving from knowledge-based benchmarks to action-based evaluation that reflects real clinical conditions.
Several implications follow for healthcare organizations and AI developers alike.
For health system leaders, MedAgentBench provides a vocabulary for evaluation that was previously absent. Rather than assessing AI vendors based on academic test performance or demo environments, procurement teams can now ask more precise questions: Has this agent been tested against FHIR-compliant workflows? What is its success rate on multi-step clinical tasks under realistic constraints? What are its documented failure modes?
For AI developers, the benchmark establishes a reproducible, open-source framework hosted at Stanford's ML Group GitHub. The environment is designed to be directly migratable to live EHR systems, which means that improvements tracked on MedAgentBench have a clear pathway to clinical relevance. The benchmark is also deliberately unsaturated-meaning current models have substantial room for improvement, and the framework can continue to drive progress as model capabilities advance.
For regulators and governance teams, MedAgentBench's safety-first design philosophy offers a model for how clinical AI should be evaluated before deployment. As the FDA increases its focus on real-world performance of AI-enabled medical devices and healthcare systems develop responsible AI frameworks, benchmarks that measure task execution rather than knowledge recall align more closely with the oversight criteria that patient safety demands.
Reducing Diagnostic Errors with Retrieval-Augmented Generation (RAG) in Clinical Decision Support. Explore the data and findings here!
Key Challenges That No Benchmark Can Solve Alone
It is worth being clear about what MedAgentBench does not address-because those gaps are as instructive as the benchmark's contributions.
MedAgentBench was developed using data from a single institution, Stanford Health Care, which means its patient profiles and clinical task distributions reflect one system's workflows, demographics, and documentation practices. Clinical AI that performs well in one health system may encounter substantially different data quality, workflow structures, and EHR configurations in another. Generalizability across institutions remains an open challenge.
The benchmark also focuses on EHR-based tasks and does not yet cover the full spectrum of clinical workflows-including real-time diagnostic support, surgical decision assistance, or mental health intervention contexts. As generative AI in healthcare expands into these domains, new evaluation frameworks will need to be developed alongside it.
Finally, even a perfect benchmark cannot substitute for the organizational change management required to deploy AI agents safely in clinical settings. Clinician training, governance structures, audit mechanisms, HIPAA compliance frameworks, and ongoing performance monitoring are all prerequisites for moving from benchmark success to patient benefit. Health systems that treat MedAgentBench scores as a deployment signal without building these surrounding structures will encounter the same "last-mile" failures that have characterized so many healthcare AI pilots to date.
Showcasing Korea’s AI Innovation: Makebot’s HybridRAG Framework Presented at SIGIR 2025 in Italy. Read here!
Conclusion
MedAgentBench arrives at a pivotal moment in the development of clinical AI workflows. The healthcare industry is no longer debating whether to adopt AI-McKinsey's data shows that 50% of U.S. healthcare organizations have already done so. The debate has shifted to a harder question: which AI deployments can actually be trusted to perform reliably in live clinical environments, with real patients and real consequences?
Stanford's answer is that trust must be earned through evidence, not assumed from benchmark scores. MedAgentBench establishes a new standard: not "does this model understand medicine?" but "can this model act within medicine's operational constraints?" Even the field's best-performing models fall short of that standard in nearly a third of tasks-not because they lack clinical knowledge, but because reliable action in complex systems requires something beyond language fluency.
The long-term implications are significant. For health systems, the benchmark provides an evaluation framework that finally aligns with clinical reality. For AI developers, it identifies clear capability gaps-FHIR API adherence, structured output reliability, multi-step task coordination-that define the roadmap for the next generation of agentic AI in healthcare. For patients and clinicians, it signals a shift toward measurable accountability in healthcare AI that the industry has long needed.
The gap between current model performance and the reliability threshold required for safe clinical deployment is not cause for pessimism-it is cause for precision. MedAgentBench has drawn the target clearly. The work now is to build systems capable of hitting it.
From Benchmark to Bedside: Build AI That Performs in Real Clinical Systems
MedAgentBench has drawn the target clearly - the next generation of healthcare AI must do more than understand medicine; it must act reliably within medicine's operational constraints. Makebot is a leading generative AI and LLM solutions provider trusted by over 1,000 enterprise clients across healthcare, public institutions, finance, and beyond. With a proprietary multi-LLM platform, a hybrid RAG architecture engineered to minimize hallucinations and output errors, and deep expertise in deploying AI that integrates directly into existing workflows - rather than operating alongside them - Makebot gives healthcare organizations the structured, governed AI foundation needed to move from promising pilots to clinical systems that meet the reliability standard that patients and clinicians actually require.
See how Makebot builds healthcare AI that works inside real workflows.






























.jpg)

.png)
















































_2.png)








