
Can AI Health Assistants Reduce Unnecessary Clinic Visits? What Early Data Suggests
AI triage tools cut unnecessary hospital visits 55% - what peer-reviewed evidence actually shows.


Introduction
Every year, millions of patients visit emergency departments and primary care clinics for conditions that could have been safely managed at home. Overcrowded waiting rooms, physician shortages, and the rising cost of in-person care have created a system under strain - one where the difference between a necessary clinic visit and an avoidable one carries real consequences for both patients and providers.
AI health assistants are entering this gap with increasing sophistication. From symptom checkers and AI-powered healthcare triage systems to conversational virtual assistants managing chronic disease, these tools are beginning to generate a credible body of evidence. Early data suggests they can meaningfully redirect care-seeking behavior - steering low-acuity patients away from emergency departments while accurately escalating those who genuinely need urgent attention.
But what does the data actually say? And where do the real-world limitations begin? This article examines the emerging evidence, the market forces accelerating adoption, and the structural challenges that will determine whether AI in healthcare fulfills its potential as a tool for reducing unnecessary clinical demand.
The Growing Role of AI Chatbots in Modern Healthcare Communication. Explore the latest insights here!
The Scale of the Problem: Why Unnecessary Visits Matter
Before evaluating AI's role, it is worth understanding the scale of what it is being asked to solve. According to McKinsey's 2024 Consumer Health Insights Survey, 25% of consumers report being unable to access care when they need it, even as emergency departments see patients who could be managed in primary care or at home. Administrative costs alone account for roughly 25% of the more than $4 trillion spent annually on U.S. healthcare - a figure that underscores how much of the system's burden is structural rather than purely clinical.
The downstream effects are significant. Industry data consistently places the average cost of a single missed appointment at approximately $200 or more in lost revenue per slot, with annual losses for a typical independent physician practice exceeding $150,000 - and substantially higher for larger multi-provider groups (MGMA, 2025). At the same time, emergency departments face growing pressure from patients presenting with non-urgent concerns - a pattern that inflates costs, delays critical care, and drives clinical burnout.
Digital health AI is positioned as a demand-side intervention: not replacing the healthcare system, but helping patients make better decisions about when, where, and how to access it.
Stanford Develops Real-World Benchmarks for Healthcare AI Agents. Read the expert analysis here!
What the Clinical Evidence Actually Shows
Symptom Checkers and Triage Redirection
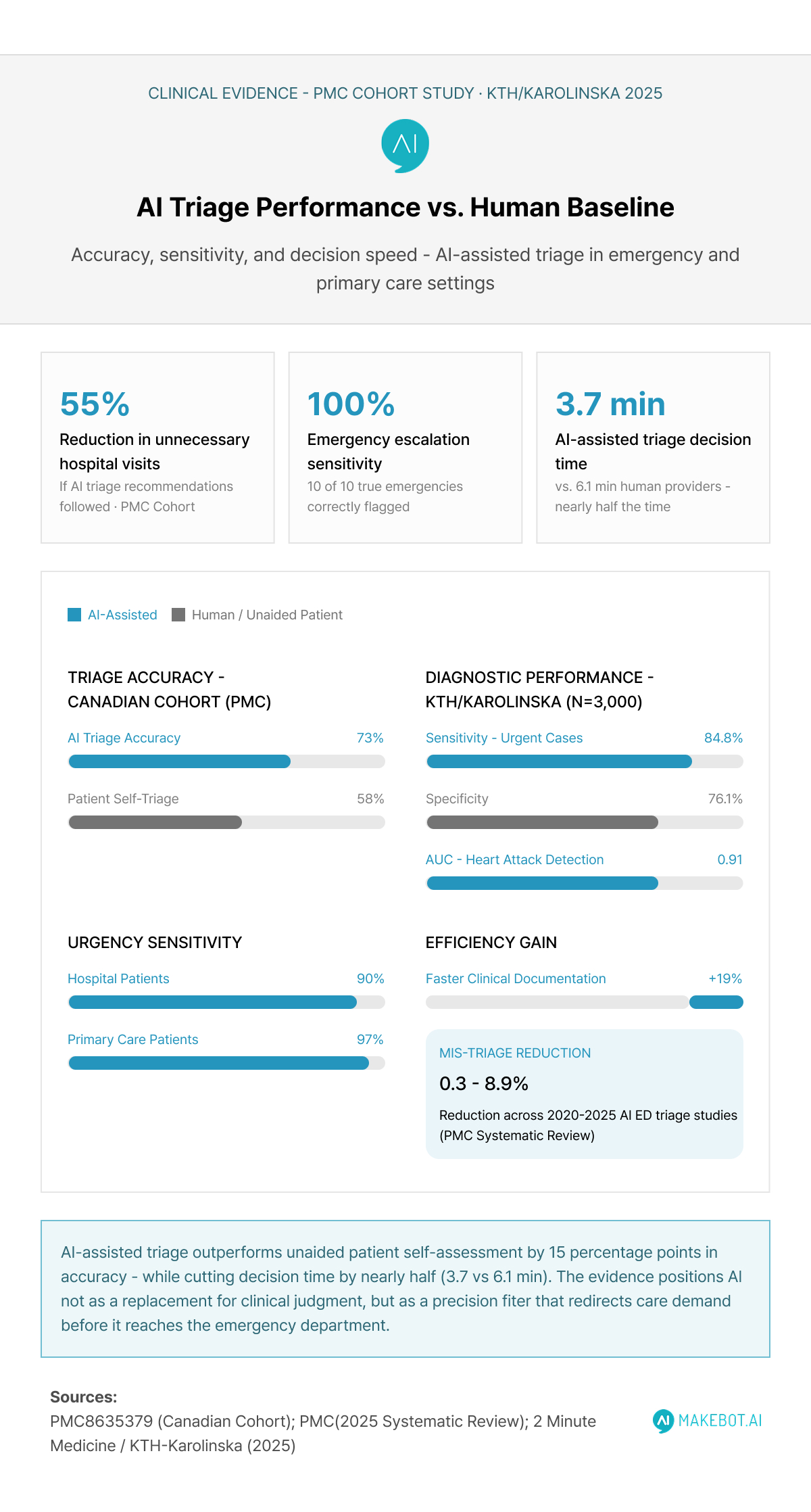
The most direct evidence for AI's impact on clinic visit reduction comes from studies evaluating AI patient support tools in triage contexts. A prospective cohort study published in PMC - one of the most frequently cited in this space - assessed a prototype symptom checker against 581 real patients presenting to hospital emergency departments and family physician clinics. The results were striking:
- The AI achieved 100% sensitivity for emergencies (10/10 cases correctly escalated)
- Sensitivity for urgent cases reached 90% in hospital patients and 97% in primary care patients
- Compliance with the AI's triage recommendations would have reduced hospital visits by 55%, though the researchers noted a 2–3% risk of delayed care for edge cases
Critically, the AI was significantly more accurate than patients attempting to self-triage (73% vs. 58%, p<0.01). This distinction matters: the question is not whether AI outperforms clinicians, but whether it outperforms the unguided health decisions patients currently make on their own.
More recent research reinforces this directional finding. A multicenter study conducted across three Swedish hospitals by researchers from KTH Royal Institute of Technology and the Karolinska Institute validated an AI-powered triage tool across nearly 3,000 real-world ED cases. The system:
- Achieved 84.8% sensitivity and 76.1% specificity in identifying urgent care needs - outperforming junior physicians
- Demonstrated an area under the curve of 0.91 for detecting heart attacks in chest pain cases
- Reduced triage decision time from a median of 6.1 minutes (human) to 3.7 minutes (AI-assisted)
A 2025 systematic review of AI-based ED triage systems (published in PMC, covering studies from 2020–2025) found that voice-based AI systems achieved 19% faster documentation versus manual methods and that machine learning algorithms reduced mis-triage rates by 0.3–8.9% across included studies - a meaningful range in contexts where misdirected care can have life-altering consequences.
Dr. Hamad Husainy on AI in Emergency Medicine: Restoring Clinical Clarity in a Data-Saturated ED. Discover what’s next here!
Remote Monitoring and the Readmission Problem
Beyond symptom checking, AI healthcare tools embedded in remote patient monitoring (RPM) platforms are demonstrating impact on a different category of unnecessary utilization: preventable hospital readmissions.
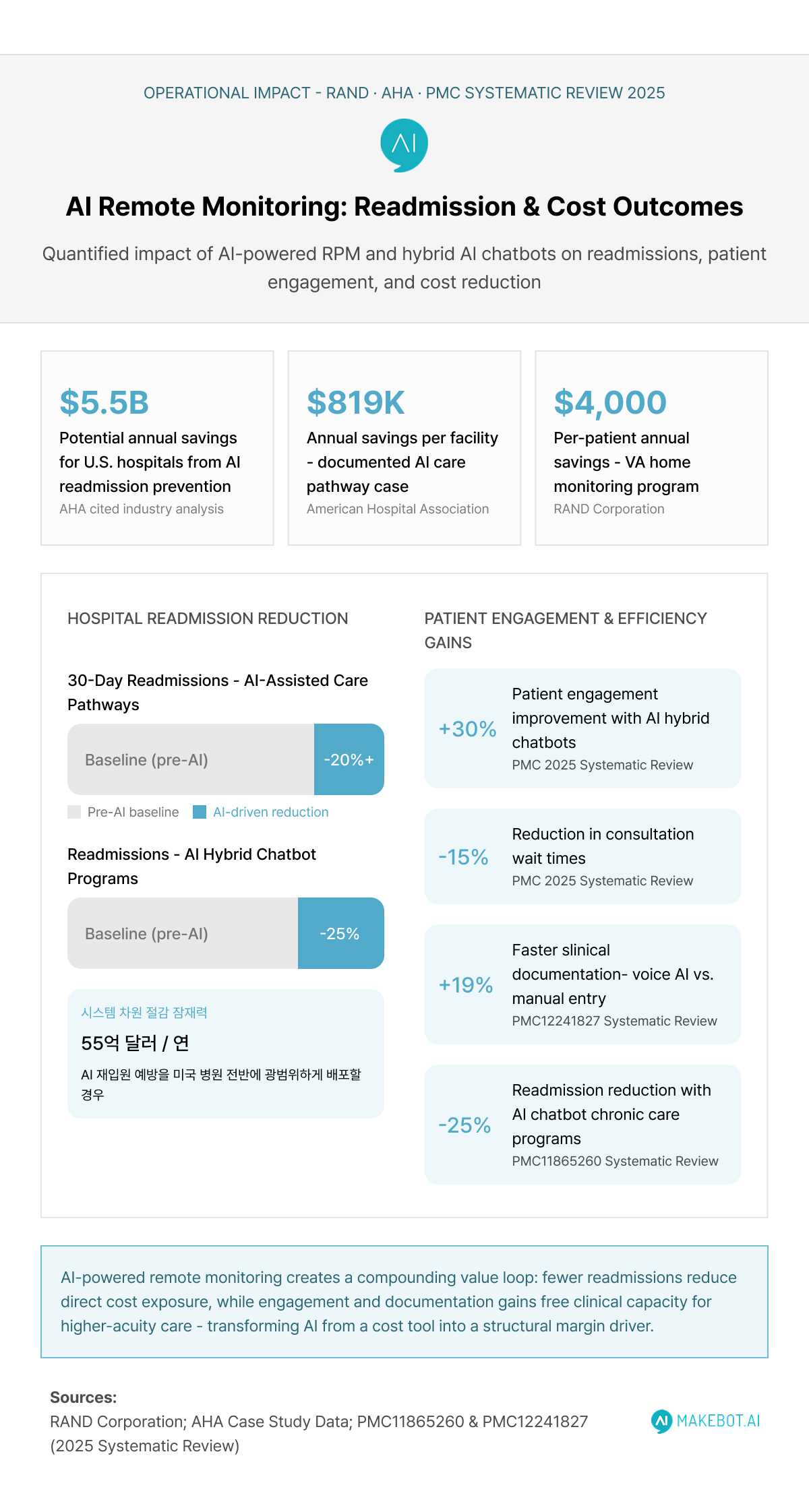
A RAND Corporation study estimated that broad use of RPM and digital health in chronic care could save the U.S. healthcare system tens of billions annually through avoided ER visits and hospital stays. One large home monitoring program for veterans documented average savings of $4,000 per patient per year.
For hospitals facing Medicare financial penalties tied to avoidable 30-day readmissions, the math is compelling. The savings evidence is compelling in documented cases: AHA case study data shows that hospitals implementing coordinated AI-assisted care pathways have reported 30-day readmission reductions exceeding 20%, with one documented program saving approximately $819,000 per facility (American Hospital Association). A separate analysis estimated that broad predictive AI deployment for readmission prevention could save U.S. hospitals $5.5 billion annually (AHA, cited by industry analysis). A peer-reviewed systematic review in PMC found that hybrid AI chatbots in healthcare settings reduced hospital readmissions by up to 25% while improving patient engagement by 30% and cutting consultation wait times by 15%.
The mechanism here is consistent: consumer healthcare AI that connects patients to remote monitoring platforms surfaces deterioration signals early and enables clinical teams to intervene before a condition escalates into an emergency admission.
LLMs as Clinical Co-Pilots (Not Decision Makers). Explore the future of AI here!
The Adoption Landscape: Where Generative AI Fits In
Rapid Institutional Uptake
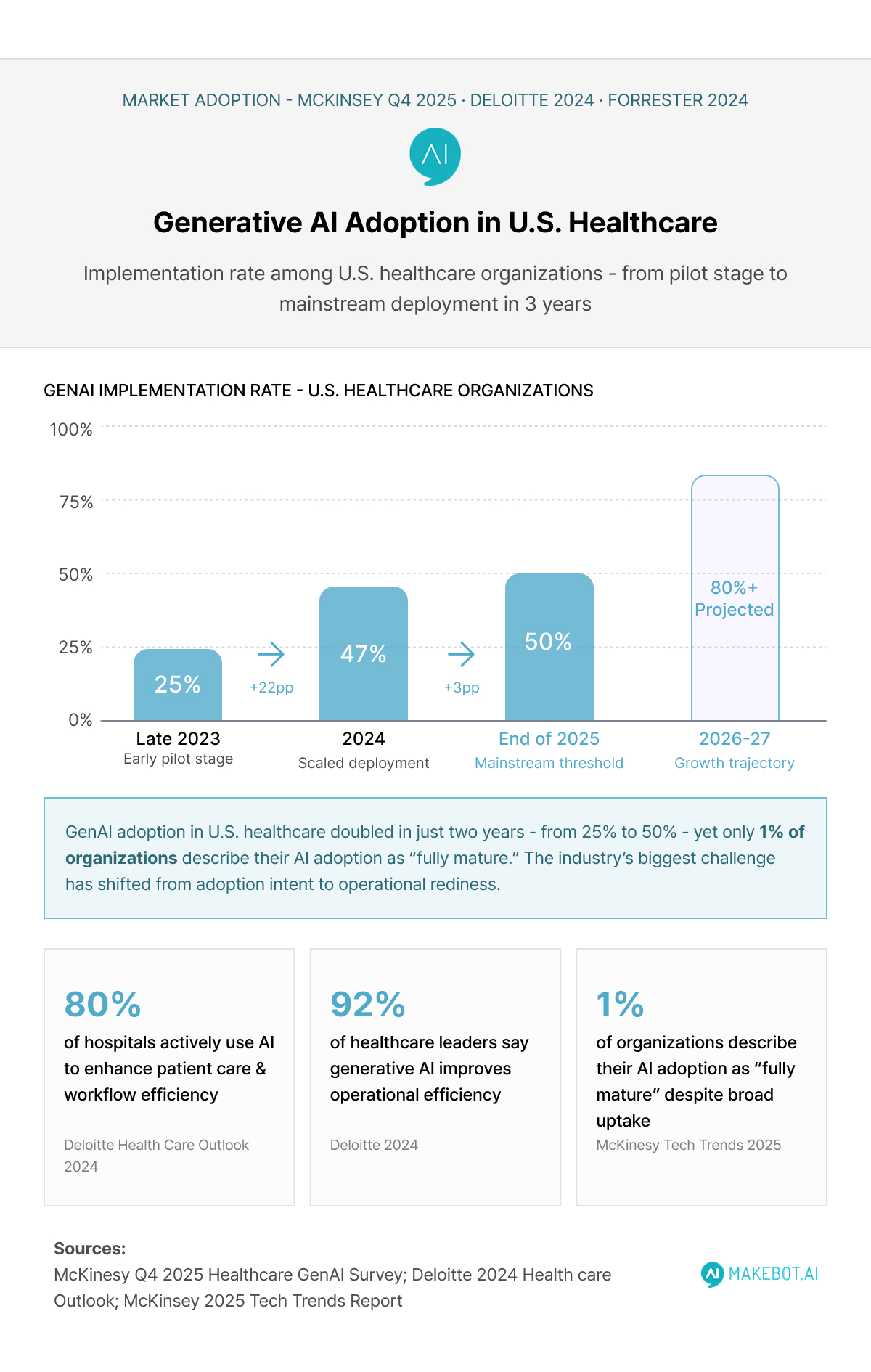
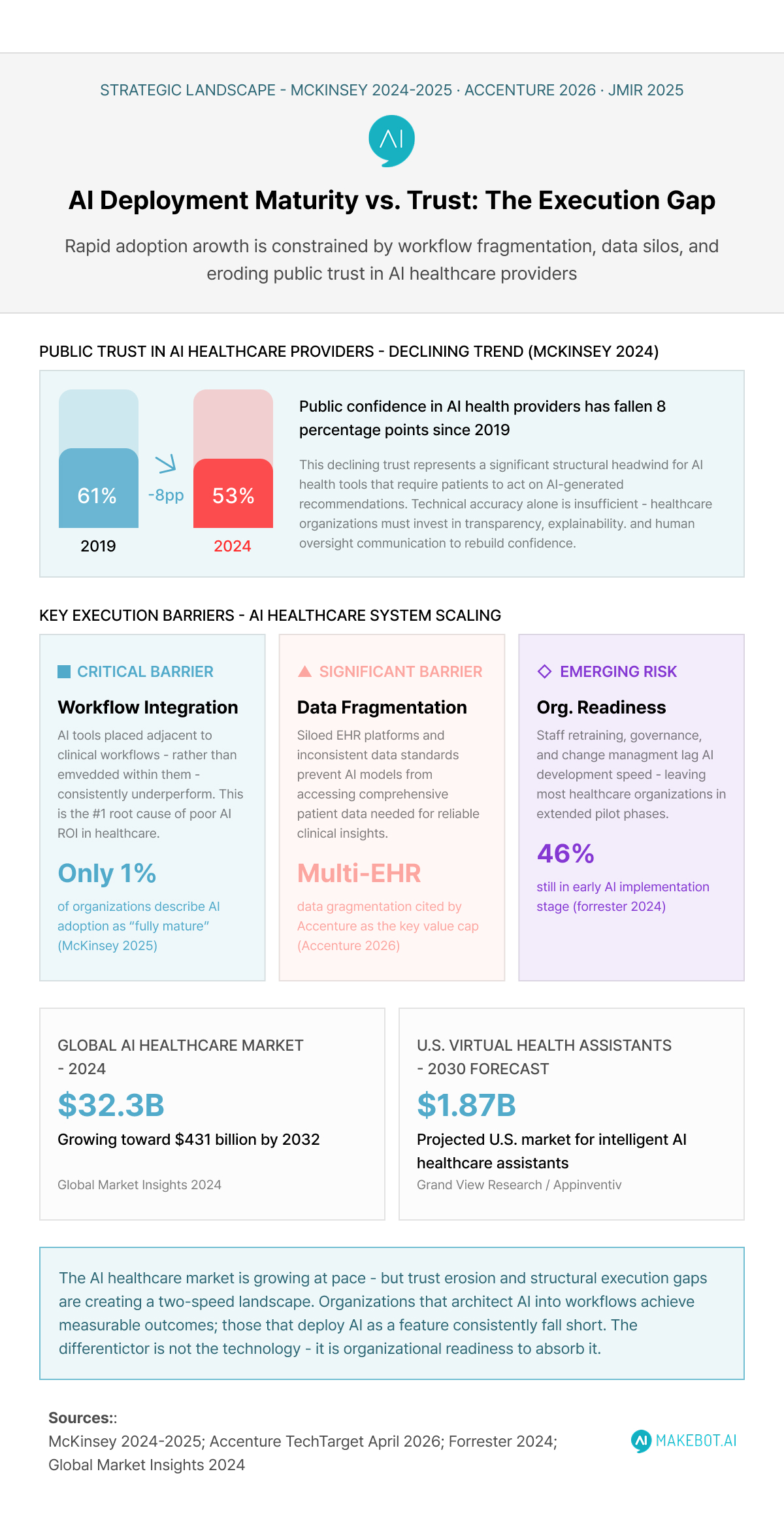
The institutional embrace of AI-powered healthcare has been one of the more dramatic technology adoption stories of the past three years. McKinsey's Q4 2025 survey of U.S. healthcare leaders revealed that 50% of healthcare organizations had implemented generative AI by the end of 2025, up from 47% in 2024 and just 25% in late 2023. More than 80% of surveyed leaders reported deploying at least one generative AI use case to end users.
Deloitte's 2024 Health Care Outlook corroborates this momentum: 80% of hospitals now use AI to enhance patient care and workflow efficiency, and 92% of healthcare leaders believe generative AI improves operational efficiency. Separately, Forrester's 2024 research found that 46% of U.S. healthcare organizations are in the early stages of generative AI implementation at the enterprise level.
The AI healthcare market grew to $32.34 billion in 2024 and is projected to reach $431.05 billion by 2032 (Global Market Insights 2024), a trajectory that reflects both clinical validation and capital confidence in the space. Within it, the U.S. market for AI healthcare assistants - including intelligent virtual health assistants - is projected to reach $1.87 billion by 2030 (Appinventiv/Grand View Research).
Consumer Behavior Is Shifting, Too
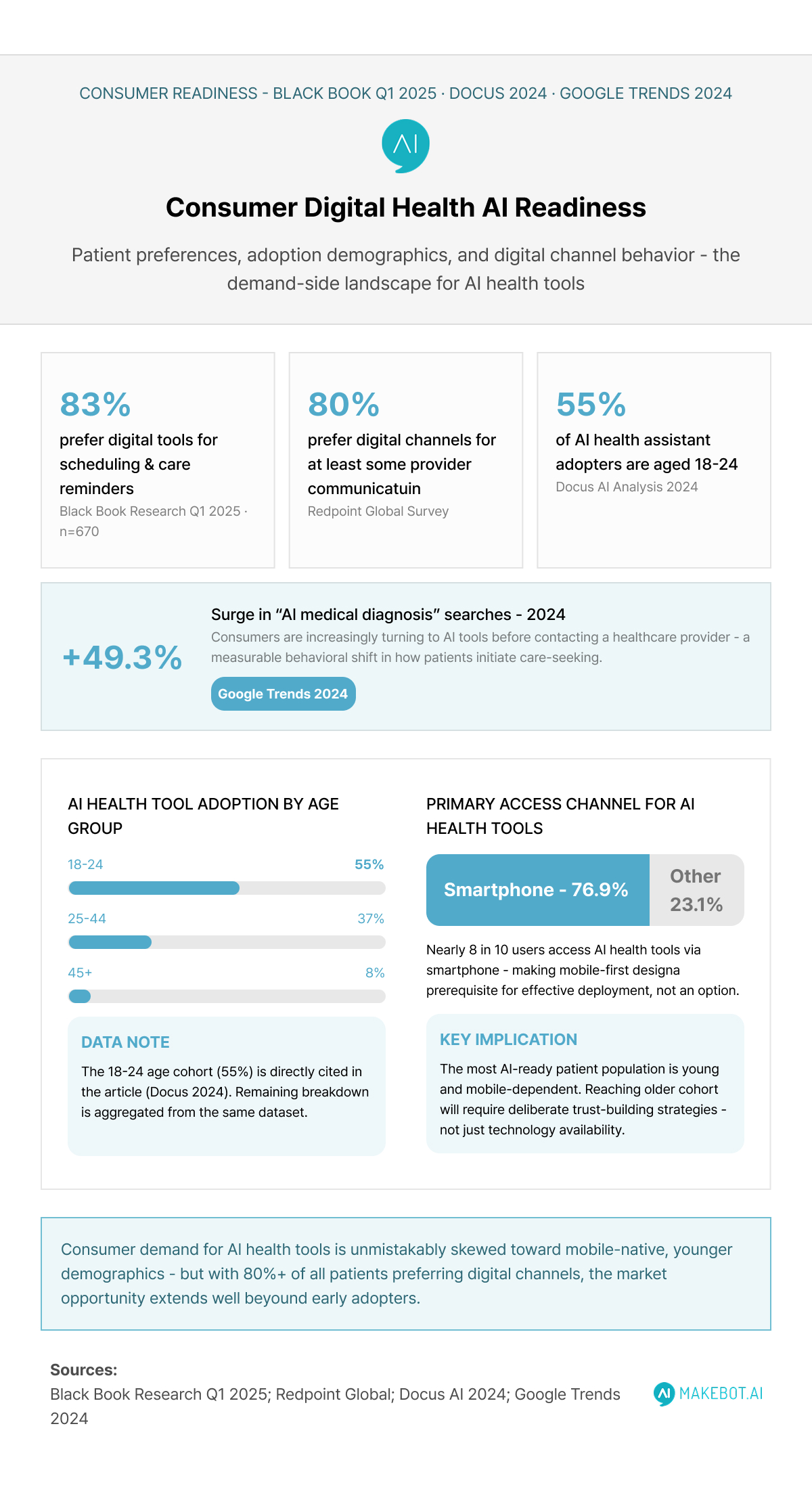
Institutional adoption tells only part of the story. Consumer behavior around AI for health advice has shifted substantially. Searches for "AI for medical diagnosis" increased by 49.3% in 2024, reflecting growing public willingness to engage AI tools before consulting a provider (Google Trends 2024). Industry surveys consistently show a strong digital preference: Black Book Research's Q1 2025 national survey of 670 healthcare consumers found that 83% prefer digital tools - such as mobile apps, portals, and reminders - for scheduling and care reminders, while separate Redpoint Global data shows 80% prefer digital channels for at least some provider communication.
The demographic profile of current consumer healthcare AI users skews younger: users aged 18–24 account for 55% of AI health assistant adoption, and 76.9% of users access these tools via smartphones (Docus 2024). This suggests that the most AI-ready patient population is also the most mobile-dependent - a dynamic that shapes both product design and go-to-market strategy for health system developers.
Key Healthcare AI Trends Shaping Innovation in 2026. See how enterprises are transforming here!
Where the Evidence Gets Complicated
The clinical and adoption data are encouraging, but honest analysis requires engaging with the limitations - not as caveats, but as structural design challenges that will determine whether AI health assistants become genuinely transformative or remain concentrated in low-complexity use cases.
The Under-Triage Risk Is Real
Both the Canadian cohort study and the 2025 systematic review of AI ED triage systems flag a consistent concern: while AI reduces overall triage errors, it can introduce under-triage risks in complex or atypical presentations. The Canadian study estimated a 2–3% potential harm rate from delayed care if patients followed AI recommendations for home management. For a tool deployed at population scale, even a small false-negative rate carries meaningful clinical stakes.
A September 2025 study published in Tandfonline assessing a Swedish digital symptom checker against real-world cases of previously erroneous telephone triage found that current evidence for digital symptom checkers remains preliminary - reinforcing that peer-reviewed validation in real patient populations, not just simulated vignettes, is necessary before large-scale deployment.
Integration and Organizational Readiness Remain Barriers
Accenture's global health AI lead captured the core operational challenge succinctly in an April 2026 TechTarget interview: "The barrier is not the availability of AI. It's organizational readiness to absorb it. The real execution gaps are workflow integration, not model performance. AI fails when it sits next to workflows instead of inside them."
McKinsey's 2025 technology trends analysis echoes this: despite broad adoption intentions, only 1% of organizations describe their AI adoption as "fully mature." Many health systems remain stuck in pilots, struggling with legacy system integration and the realities of retraining staff. A 2024 Wolters Kluwer survey found many physicians eager to use AI but reporting their organizations hadn't yet prepared for deployment.
Data fragmentation compounds these challenges. As Accenture's analysis notes, fragmented data and inconsistent standards adoption can cap the value of even sophisticated AI models - a particular concern in healthcare environments where patient data spans multiple EHR platforms, payer systems, and care settings.
Trust Erosion Is a Strategic Concern
Perhaps the most underappreciated challenge for generative AI in healthcare is the erosion of public trust in AI providers more broadly. McKinsey's tracking data shows public confidence in AI providers fell from 61% in 2019 to 53% in 2024 - a decline that matters significantly in a domain where patients are making consequential health decisions based on AI-generated recommendations.
A 2025 Journal of Medical Internet Research study on trust and AI acceptance in healthcare found that hesitancy toward chatbots correlated with IT skill levels and discomfort with non-human interaction. In clinical and consumer AI adoption alike, accuracy, transparency, and explainability are cited as decisive barriers - particularly among populations without prior exposure to AI tools.
For health systems deploying AI healthcare assistants, this means that technical performance alone will not drive adoption. Trust architecture - encompassing how AI recommendations are explained, how errors are surfaced, and how human oversight is communicated - is as important as model accuracy.
Health System Execs Are Prioritizing AI. Learn how industry leaders are adapting here!
The Opportunity Architecture: What Success Looks Like
Despite these challenges, the structural case for AI patient support at scale is strong. The conditions that produce meaningful outcomes - reduced unnecessary visits, lower readmissions, better triage accuracy - share a common profile:
- AI embedded in workflow, not adjacent to it (AI-assisted clinical decision support vs. standalone chatbot)
- Continuous monitoring integration, particularly for chronic disease populations where readmission risk is highest
- Human oversight at decision escalation points, ensuring the AI serves as a safety net rather than a replacement for clinical judgment
- Patient-facing design that builds trust, with clear communication about what the AI can and cannot reliably assess
The most compelling evidence - the 55% reduction in unnecessary hospital visits, the 20% drop in readmissions, the $4,000 per-patient annual savings in VA home monitoring - comes from implementations that meet most of these criteria. The least compelling outcomes come from deployments where AI-powered tools are added to existing workflows without redesigning those workflows around their actual capabilities.
Showcasing Korea’s AI Innovation: Makebot’s HybridRAG Framework Presented at SIGIR 2025 in Italy. Read here!
Conclusion
The early data on AI health assistants and unnecessary clinic visits tells a coherent, if cautious, story. The potential is real: peer-reviewed evidence points to substantial reductions in avoidable hospital visits, meaningful improvements in triage accuracy, and measurable cost savings across readmission prevention and remote monitoring programs. The market is responding accordingly - $32.34 billion in 2024, on a trajectory toward $431 billion by 2032.
But the gap between potential and consistent, scaled delivery remains significant. The organizations achieving strong outcomes are those that treat AI deployment as a workflow redesign challenge, not merely a technology procurement decision. Where these tools sit inside clinical processes - informing decisions, escalating risk, supporting patients between visits - the evidence is compelling. Where they sit outside those processes, as stand-alone apps or disconnected chatbots, the evidence is thinner.
For health system leaders, the strategic priority is clear: AI in healthcare cannot be treated as a feature to be added. It needs to be architected into the patient journey - from initial symptom assessment through chronic disease monitoring and care navigation. The clinical evidence, while still maturing, is already strong enough to justify serious investment. The question is no longer whether AI health assistants can reduce unnecessary clinic visits. It is whether organizations can build the operational infrastructure to let them.




























.jpg)

.png)
















































_2.png)










