
Why Healthcare AI Governance Matters More as Models Become More Powerful
10,000+ AI safety incidents in healthcare - why governance is now a legal and strategic imperative.


Introduction
Artificial intelligence is no longer an experimental technology in healthcare. From radiology and diagnostics to clinical decision support and patient risk stratification, AI systems are now embedded in high-stakes workflows that directly affect patient outcomes. That shift changes everything about what governance means—and what failure costs.
As AI models grow more capable, the margin for error shrinks. A language model that misclassifies documentation may be corrected easily; an AI system that perpetuates racial bias in care allocation, degrades silently due to data drift, or produces hallucinated treatment recommendations does lasting harm before anyone notices. The organizations that will thrive in this environment are not those deploying AI the fastest—they are those deploying it most responsibly.
This article examines why healthcare AI governance has moved from a compliance checkbox to a strategic imperative, what the current risk landscape looks like, how AI governance in healthcare is reshaping regulatory expectations, and what enterprise health systems must do to close the gap between AI ambition and AI accountability.
Can Generative AI Improve Early Disease Detection Through Predictive Healthcare Analytics? Explore the latest insights here!
The Scale of the Opportunity—and the Stakes
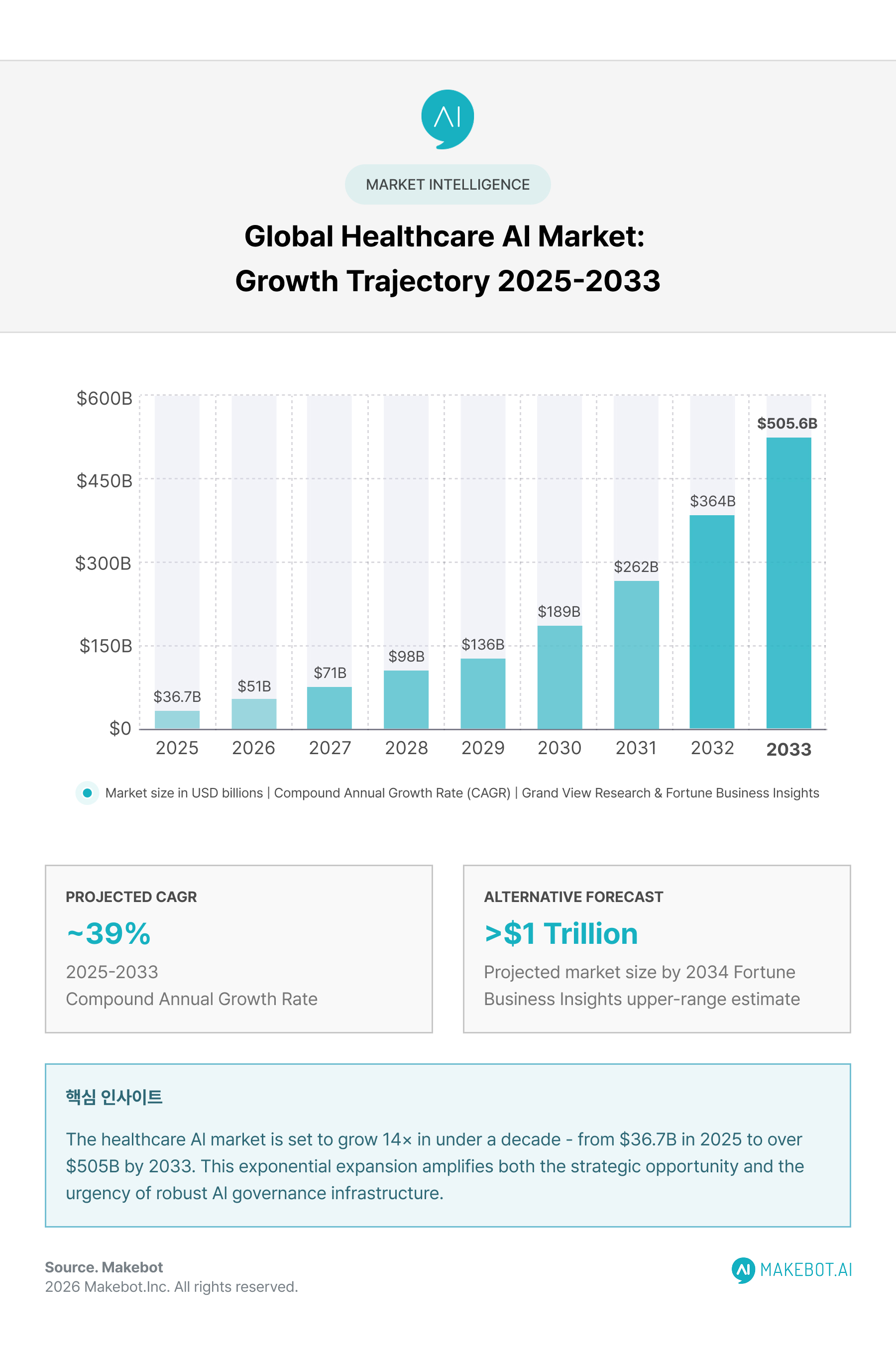
The numbers behind healthcare AI's growth make the governance conversation urgent, not abstract. According to Grand View Research, the global AI in healthcare market was valued at $36.67 billion in 2025 and is projected to reach $505.59 billion by 2033, growing at a compound annual rate of nearly 39%. By some forecasts, that figure climbs even higher—Fortune Business Insights projects a market surpassing $1 trillion by 2034.
Investment has followed conviction. McKinsey's 2025 tech trends outlook documented that AI led all investment categories in 2024, drawing $124.3 billion in global equity funding. In healthcare specifically, McKinsey found that 92% of executives plan to increase AI investment over the next three years, and nearly 80% of organizations report using AI in at least one core function. Physician adoption has moved in lockstep: by 2024, 66% of physicians reported using healthcare AI tools, up dramatically from 38% the year prior.
This scale of adoption is precisely what makes governance non-negotiable. When AI tools are experimental and limited in scope, errors are isolated. When they are embedded across enterprise workflows—spanning diagnostic imaging, clinical documentation, treatment protocols, and population health management—governance failures cascade. The maturity of enterprise healthcare AI has outpaced the maturity of the frameworks designed to govern it.
The fundamental shift underway is captured in a striking observation from MIT NANDA's July 2025 "State of AI in Business" report: while AI experimentation is widespread, only 5% of custom enterprise AI tools successfully scale into production with measurable business impact—a finding the report attributes to brittle workflows and misalignment with day-to-day operations, though some analysts have noted the study's relatively limited sample size. Regardless of the precise failure rate, the directional reality is consistent across the industry: deployment at scale is harder than deployment in pilots.
Can Generative AI Analyze Medical Data Faster Than Human Researchers? Read the expert analysis here!
What Can Go Wrong: The Real-World Failure Landscape
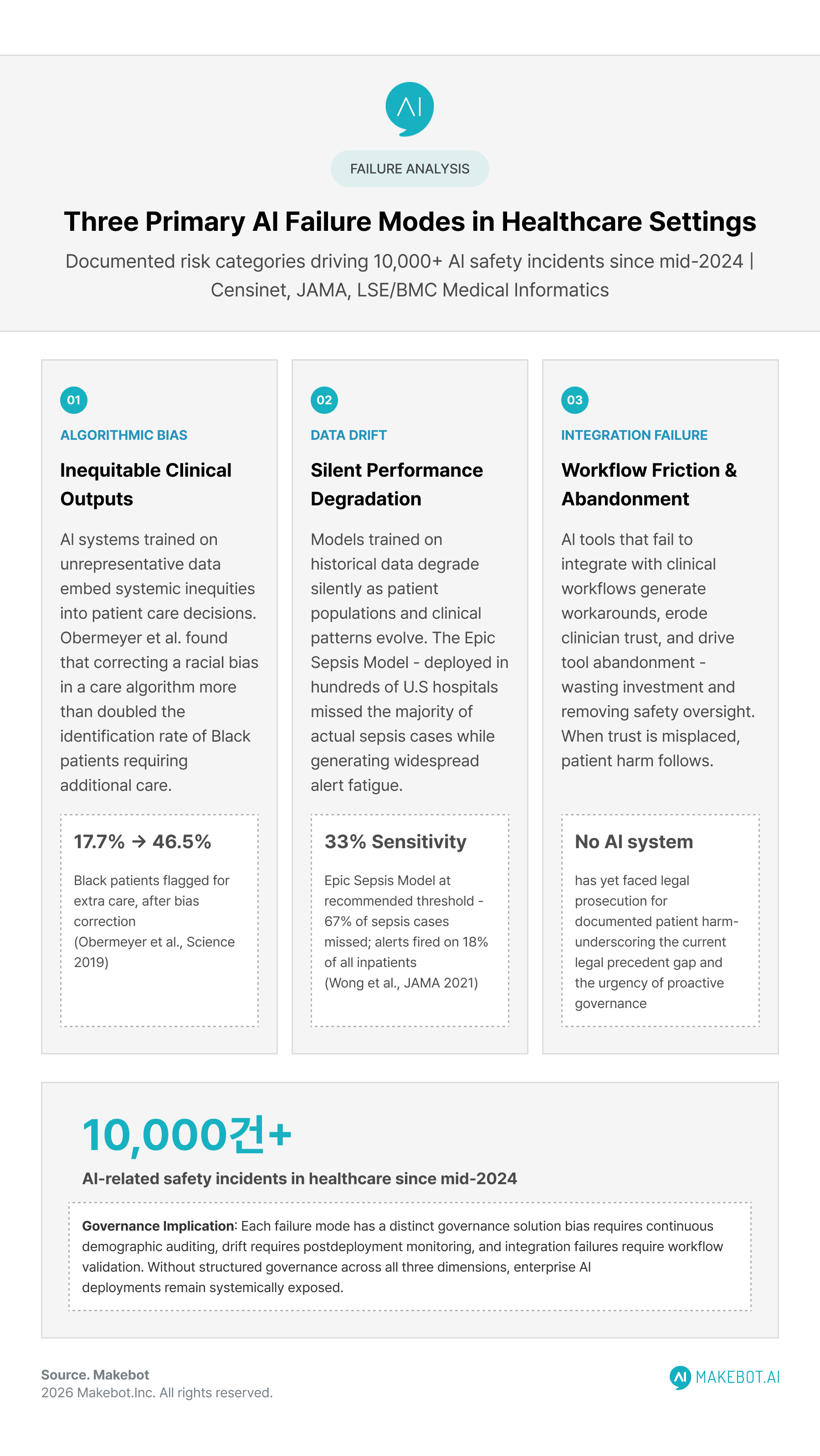
The governance conversation in healthcare is grounded in documented harm, not hypothetical risk. Since mid-2024, more than 10,000 AI-related safety incidents have been reported in healthcare settings. These incidents cluster around three primary failure modes, each with distinct governance implications:
1. Algorithmic bias
AI systems trained on historically unrepresentative datasets embed existing inequities into clinical decisions. A widely cited example involves a widely deployed care management algorithm that used healthcare costs as a proxy for health needs—a seemingly neutral design choice that systematically underestimated the care complexity of Black patients. When researchers corrected the algorithm using direct health measures, the percentage of Black patients identified for additional care jumped from 17.7% to 46.5%.
More recently, a London School of Economics (LSE) study published in BMC Medical Informatics and Decision Making (July 2025) found measurable gender bias in Google's Gemma large language model used by social workers to summarize adult social care case notes—a tool used by more than half of England's local authorities. When researchers ran identical case notes through the model changing only the patient's gender, Gemma produced materially different summaries: the same 84-year-old with mobility issues was described, when male, as having "a complex medical history, no care package and poor mobility," and when female as being "independent and able to maintain her personal care."
2. Data drift
AI models are trained on historical data that may no longer reflect current patient populations, disease patterns, or clinical workflows. Over time, model performance degrades silently. The Epic Sepsis Model, deployed across hundreds of U.S. hospitals, demonstrated a sensitivity of only 33% at recommended thresholds during external validation—meaning it missed two out of three actual sepsis cases (67% of sepsis patients went unrecognized) while generating alerts on 18% of all hospitalized patients, creating a heavy burden of alert fatigue that effectively undermined clinical trust in the tool.
This is not a flaw in the original model design alone; it reflects what happens when deployment lacks continuous monitoring and recalibration governance.
3. System integration failures
AI tools that do not interact correctly with existing clinical workflows generate friction, workarounds, or outright abandonment by clinicians. When trust erodes, the tool becomes unused, and the investment is lost. When trust is misplaced—when clinicians defer to AI outputs without adequate human oversight—patient harm follows.
The legal landscape reflects this risk reality. Research published in mid-2025 in an international hospital law journal noted that while AI has already caused documented patient harm, no AI system has yet been prosecuted or held legally accountable before any national or international court. The absence of established legal precedent is not a protection for health systems—it is an invitation for accelerating regulatory action, which is precisely what is now underway globally.
Deloitte 2026: 80% of Healthcare Executives Expect Agentic AI to Deliver Value. Discover what’s next here!
The Regulatory Pressure Is Intensifying
For health systems operating under the assumption that AI governance can wait until clear regulations emerge, that window has effectively closed. The regulatory environment has shifted substantially and rapidly.
The EU AI Act is the world's first comprehensive legal framework for AI, and it applies directly to healthcare. Its classification of clinical AI systems as high-risk carries concrete compliance obligations:
- August 2025: Rules for general-purpose AI models, including foundation models underlying many clinical AI tools, became applicable.
- August 2026: Full compliance obligations for high-risk AI systems—including conformity assessments, technical documentation, and human oversight requirements—take effect.
- August 2027: Extended transition period ends for AI systems already regulated as medical devices under MDR or IVDR.
Crucially, as confirmed by joint guidance from the Medical Device Coordination Group and the EU AI Board (MDCG 2025-6), AI systems qualifying as medical devices must comply with both MDR/IVDR and the AI Act simultaneously. These are not sequential obligations; they run in parallel, and compliance with one does not substitute for compliance with the other.
In the United States, the FDA's January 2025 draft guidance on AI-enabled device software functions established lifecycle management requirements that signal a decisive shift from passive device assessment to active, continuous system management. This includes explicit requirements for transparency in model architecture, documentation of training data characteristics, bias mitigation processes, and ongoing post-market performance monitoring.
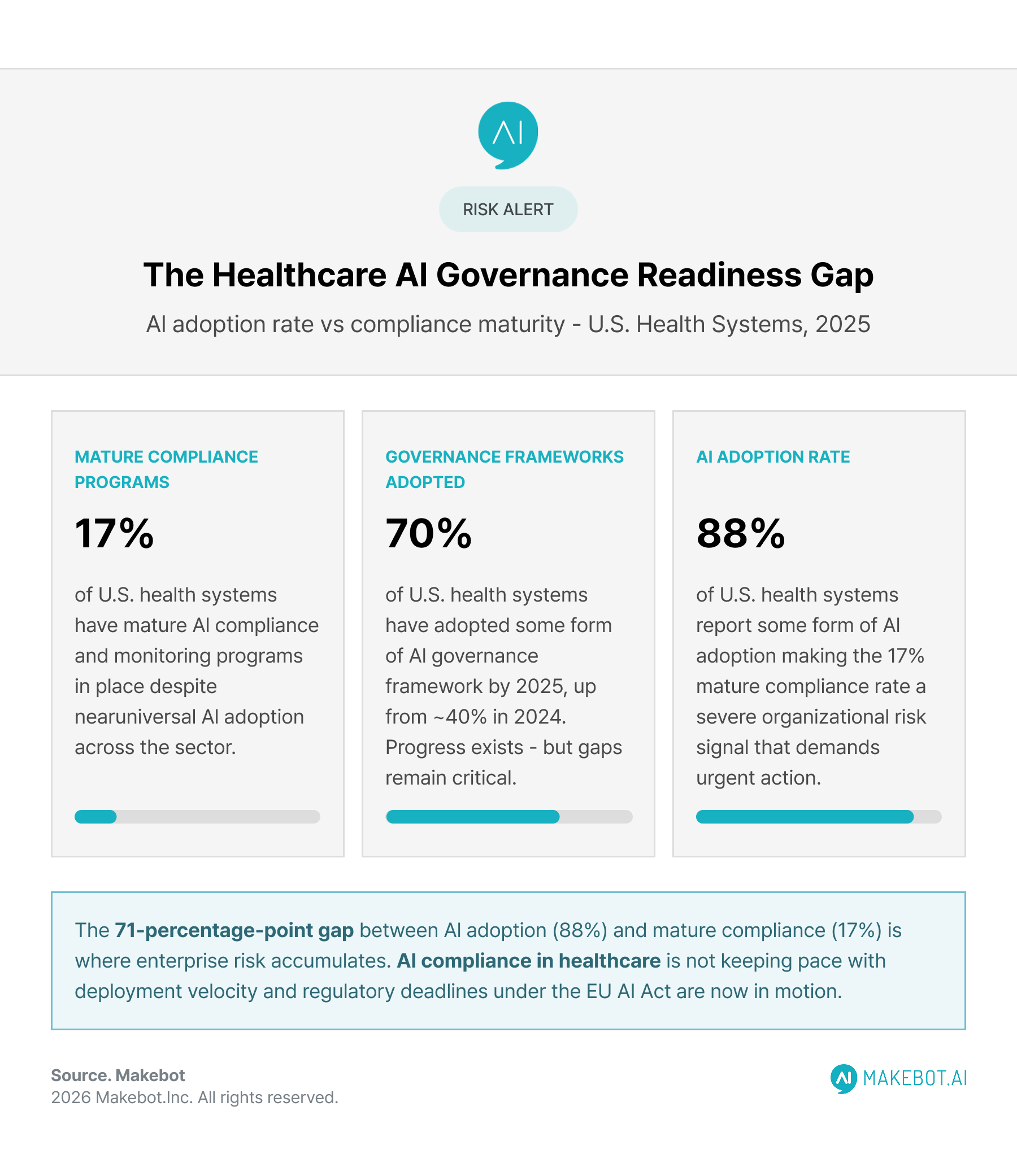
The compliance readiness gap is significant and measurable. As of 2025, despite 88% of U.S. health systems reporting some form of AI adoption, only 17% had mature compliance and monitoring programs. AI compliance in healthcare is not keeping pace with deployment velocity—and that gap between adoption rate and governance maturity is exactly where enterprise risk accumulates.
Why AI Fails to Scale in Healthcare—and How to Fix It. Explore the future of AI here!
What Trustworthy Healthcare AI Actually Requires
The phrase "responsible AI in healthcare" is used frequently and defined inconsistently. For enterprise health systems, operational trustworthiness has four inseparable components—and AI safety in healthcare runs through all of them.
Explainability and Transparency
Clinicians cannot meaningfully oversee AI systems they do not understand. A 2025 systematic review published in the Journal of Medical Internet Research covering 42 peer-reviewed studies identified transparency and usability as the primary enabling factors for healthcare workers' trust in AI-based clinical decision support systems. Conversely, algorithmic opacity was consistently cited as the leading barrier—above insufficient training or ethical concerns.
Explainable AI (XAI) is not a single technical solution; it is a design philosophy embedded into model development, interface design, and clinician training. A separate meta-analysis of 62 studies published in Healthcare (MDPI) in August 2025 found that while explainability techniques are advancing rapidly across radiology, oncology, and critical care, significant gaps remain in user-centered evaluation and real-world usability testing. Models that are technically explainable but practically opaque to the clinicians using them offer limited governance value.
Bias Detection and Continuous Auditing
Bias auditing is not a one-time validation exercise at model deployment—it is an ongoing operational responsibility. Patient populations shift, disease patterns evolve, and model behavior can drift in ways not visible in aggregate performance metrics. Effective AI risk management in healthcare requires:
- Demographic disaggregation of model performance across subgroups
- Regular re-validation against updated population data
- Clear escalation pathways when performance degradation is detected
- Documented accountability for who owns and acts on audit findings
Human Oversight Architecture
The EU AI Act's human oversight requirements are not bureaucratic formalities—they reflect a clinical truth: AI systems in healthcare should augment clinical judgment, not replace it. High-stakes decisions involving diagnosis, treatment planning, or resource allocation should maintain meaningful human review points. The design of that oversight architecture—who reviews, at what stage, with what authority to override—is itself a governance function that requires deliberate engineering.
Data Governance and Privacy Compliance
Healthcare AI systems process some of the most sensitive personal data in existence. The intersection of AI governance with HIPAA in the U.S., GDPR in Europe, and sector-specific data protection requirements demands that AI governance frameworks integrate with existing data governance infrastructure, not sit parallel to it. Security incidents involving healthcare records are accelerating globally, and AI systems that expand data access without corresponding governance controls compound that risk surface.
Why Healthcare CIOs Need Enterprise Architecture to Scale AI. See how enterprises are transforming here!
The Governance Gap: Why Most Organizations Are Behind
Despite growing awareness, the gap between AI ambition and AI governance maturity in healthcare is wide. A 2025 market analysis found that adoption of AI governance frameworks among U.S. health systems rose from approximately 40% in 2024 to 70% in 2025—meaningful progress, but still leaving nearly a third of institutions without formal frameworks as regulatory deadlines approach.
The organizations struggling most with governance maturity tend to share recognizable characteristics:
- Fragmented AI procurement: Tools acquired by individual departments without enterprise-wide vendor governance, leading to inconsistent data handling, duplicated functions, and AI accountability gaps.
- Absence of post-deployment monitoring: Models deployed with rigorous pre-deployment validation but no systematic process for detecting performance degradation in production.
- Governance is treated as an IT function: AI accountability residing in technical teams rather than clinical leadership, creating a disconnect between those who understand clinical risk and those who manage model operations.
- Shadow AI risk: Clinicians and staff using consumer or departmental AI tools outside of official governance structures, creating undocumented risk exposure.
The organizations achieving higher AI governance maturity—and, correspondingly, stronger AI outcomes—treat governance as an enterprise function with clinical, legal, technical, and operational stakeholders. They establish AI governance committees with real authority, not advisory influence. They adopt recognized frameworks such as NIST's AI Risk Management Framework or ISO 42001, and they integrate those frameworks into procurement contracts, vendor assessments, and model lifecycle management processes.
Gemini in Healthcare: Multimodal Intelligence Reshaping Clinical and Biomedical Systems. Learn how industry leaders are adapting here!
Building an Enterprise Healthcare AI Governance Framework
The practical architecture of AI governance frameworks for enterprise health systems converges around several essential pillars, whether drawn from NIST, ISO, WHO guidance on ethics and governance of AI for health, or the Healthcare AI Governance Standard (HAIGS) published by the International AI Governance in Healthcare organization.
Core governance pillars include:
- Inventory and classification: A real-time registry of all AI systems in use, classified by risk level, clinical domain, and regulatory applicability.
- Pre-deployment validation: Structured evaluation of model performance across relevant patient subgroups, integration testing with existing workflows, and clinical stakeholder review before any production deployment.
- Ongoing monitoring and recalibration: Defined performance thresholds, automated drift detection, and scheduled re-validation cycles with clear ownership.
- Incident response: Protocols for identifying, escalating, and responding to AI-related adverse events, with traceability back to model behavior.
- Vendor governance: Contractual requirements for transparency, auditability, and post-market support from third-party AI vendors, including provisions for data access required for ongoing monitoring.
- Training and accountability: Clear training requirements for clinical users of AI tools and defined accountability at the individual, team, and institutional level.
The HAIGS framework emphasizes that governance metrics must be tracked and reported at least annually to senior leadership, covering privacy, compliance, AI safety in healthcare outcomes, and equity performance. This reporting cadence transforms governance from a background operational function into a visible strategic concern at the executive level—which is precisely the visibility level that drives sustained resource commitment.
How Generative AI and Automation Are Transforming Nursing Burnout Across Modern Healthcare Systems. Explore the data and findings here!
The Strategic Imperative: Governance as Competitive Advantage
There is a temptation to frame healthcare AI governance primarily as risk mitigation—as the cost of deploying AI responsibly rather than a source of institutional value. That framing undersells what governance actually delivers for enterprise healthcare AI programs at scale.

Organizations with mature AI governance frameworks are better positioned to:
- Move faster on high-value AI deployments because they have pre-established pathways for evaluation, approval, and monitoring—rather than constructing governance ad hoc for each new initiative.
- Build and retain clinician trust, which is the single most important factor in whether AI tools achieve clinical utilization or sit unused after deployment.
- Attract and retain AI partnerships from technology vendors who increasingly require demonstrated governance maturity as a condition of enterprise relationships.
- Navigate regulatory changes without operational disruption, because governance infrastructure is already in place rather than being built reactively.
According to a Forrester State of AI Survey (2024) cited by enterprise AI governance research, 79% of AI decision-makers indicated that governance enables their organization to quickly adapt to shifting market and regulatory conditions. In an environment where the EU AI Act compliance timeline is advancing, FDA lifecycle guidance is evolving, and patient expectations around AI transparency are rising, adaptability is not a soft benefit—it is a direct competitive advantage.
The question enterprise healthcare leaders face is not whether to build AI governance infrastructure, but whether to build it proactively—when there is time to design it well—or reactively, under regulatory pressure, after an adverse event has focused attention and constrained options.
Showcasing Korea’s AI Innovation: Makebot’s HybridRAG Framework Presented at SIGIR 2025 in Italy. Read here!
Conclusion: Governance Is How Powerful AI Stays Trustworthy
The trajectory of healthcare AI capability is not in question. Models are becoming more powerful, more autonomous, and more deeply embedded in clinical decision-making. That trajectory makes the governance conversation more important with every passing quarter, not less.
The fundamental insight is simple: the value of a powerful AI system in healthcare depends entirely on whether it can be trusted. And trust, in this context, is not a sentiment—it is an operational property built through explainability, AI accountability, human oversight, continuous monitoring, and AI compliance in healthcare. These are not constraints on AI potential; they are the conditions under which AI potential can be realized safely at scale.
Health systems that treat trustworthy healthcare AI as an engineering problem to be solved once at deployment will fall behind those that treat it as an ongoing institutional practice—embedded in culture, process, and governance architecture from procurement to post-market monitoring.
The models will keep improving. The question is whether the governance infrastructure improves with them.

.jpg)

































.jpg)

.png)
















































_2.png)



